Clinical guidelines for MRONJ are based on the latest research from global authorities. However, medical science in this area is still a “moving target.” Recommendations regarding “drug holidays,” surgical techniques, and new “booster” medications are updated frequently as new data emerges from different international task forces.
This guide synthesizes the most recent data from the American Association of Oral and Maxillofacial Surgeons (AAOMS) (2022), the Italian National Consensus (2024), the Japanese Revised Position Paper (2024), and the Korean Consensus (2025).
Always consult with your specific multidisciplinary team (Dentist, Oral Surgeon, and Oncologist/Rheumatologist) for the most current advice tailored to your unique health profile.
1. What exactly is MRONJ?
(Medication-related osteonecrosis of the jaw: definition and best practice for prevention, diagnosis, and treatmentNicolatou-Galitis, Ourania et al.Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, Volume 127, Issue 2, 117 – 135)
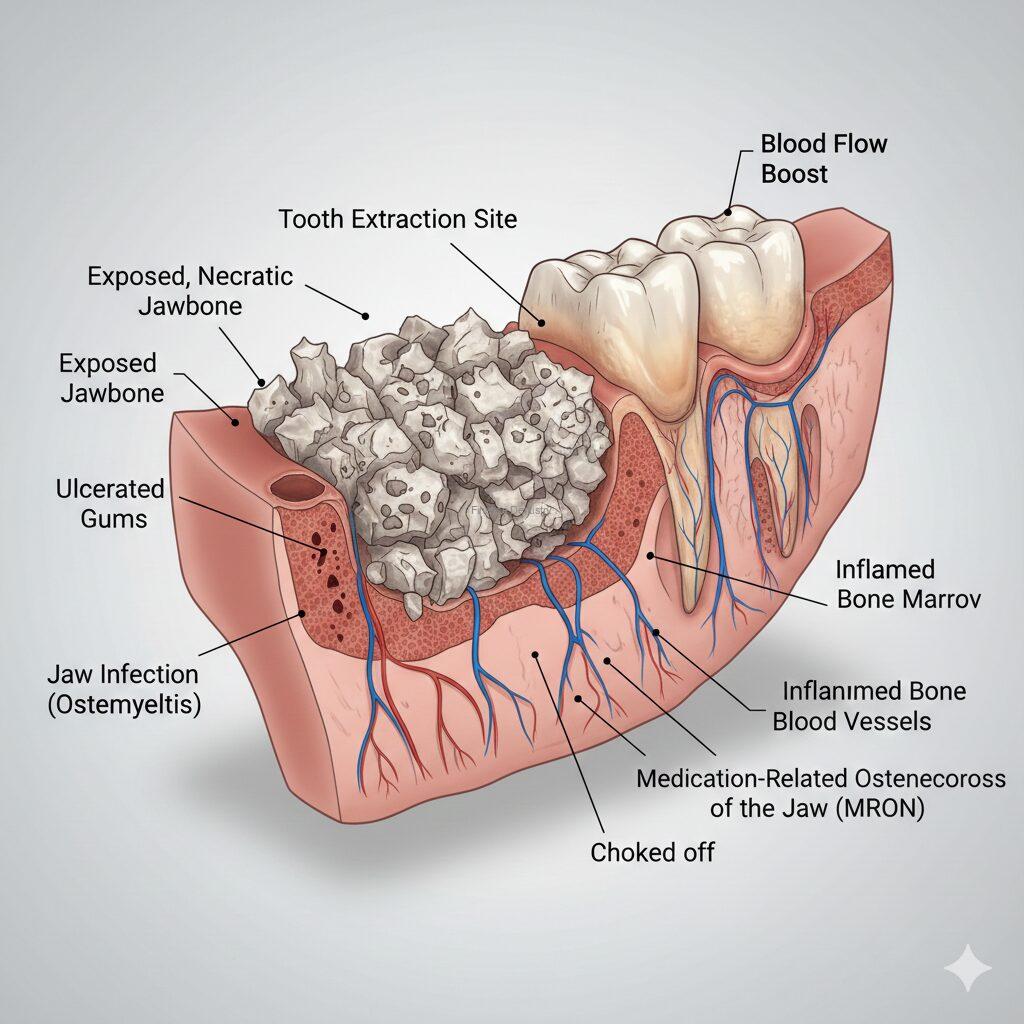
MRONJ stands for Medication-Related Osteonecrosis of the Jaw. It is a condition where an area of the jawbone fails to heal and remains “exposed” (you can see or feel the bone through your gums) for more than 8 weeks.
- The Evolution: Originally known as BRONJ (limited to Bisphosphonates), the American Association of Oral and Maxillofacial Surgeons (AAOMS) expanded the term to MRONJ in 2014 to include other agents like denosumab and anti-angiogenics that also affect the jaw.
2. Which medications are the main “culprits”?
It is not just one drug. The risk depends on the dose and the reason for treatment:
- Bisphosphonates: (e.g., Fosamax, Reclast, Zometa).
- RANKL Inhibitors: (e.g., Prolia, Xgeva).
- Anti-angiogenics: Certain cancer drugs that stop blood vessel growth (e.g., Bevacizumab/Avastin®, Sunitinib/Sutent®).
- Note: The risk is significantly higher for patients receiving high doses for cancer treatment than for those taking them for osteoporosis.
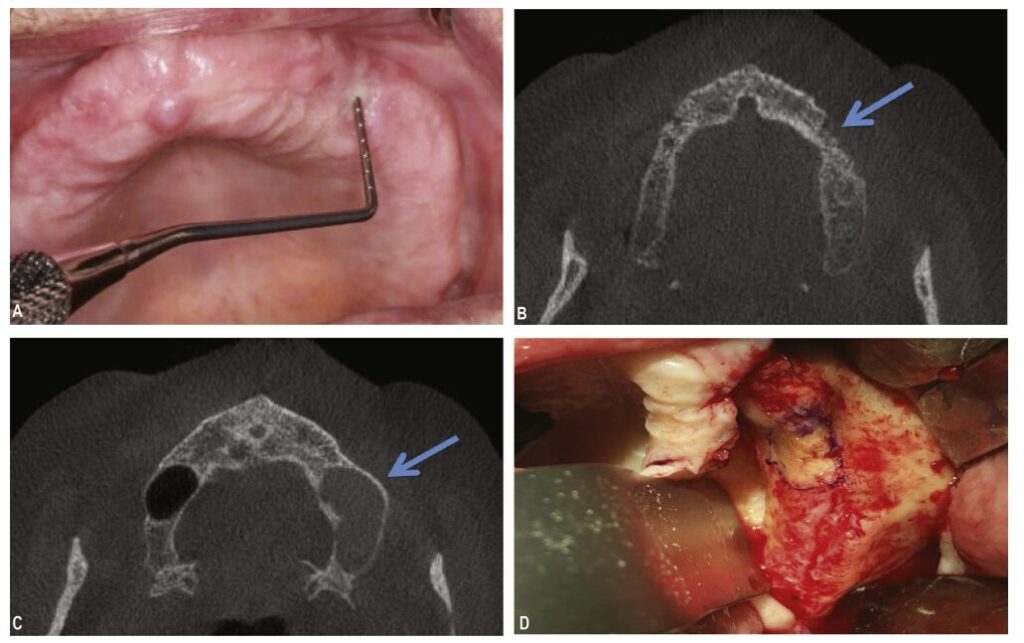
3. Why is my dentist asking for a 3D Scan (CBCT)?
Standard 2D X-rays often miss early signs. The 2024 Italian National Consensus (SIPMO-SICMF) and the 2025 Korean Consensus strongly advocate for advanced imaging.
- The Benefit: A CBCT (3D Dental Scan) allows surgeons to see inside the bone. The Italian guidelines emphasize that internal bone changes on a CT scan can confirm a diagnosis even if the bone isn’t visible through the gums yet (referred to as Stage 0).
4. Should I take a “Drug Holiday” before dental work?
A “drug holiday” is a temporary pause in your medication. International opinions vary:
- The AAOMS (2022) View: Suggests this is an option to discuss with your doctor; there is no “one-size-fits-all” proof it prevents MRONJ.
- The Japanese Revised Paper (2024): Maintains a cautious view, noting limited evidence that a holiday prevents MRONJ and warning of increased fracture risks.
- The Korean Update (2025): Offers specific timing—suggesting oral pill users consider a 2-month pause, and Prolia users time surgery 3 to 4 months after the last injection.
5. Is there a “cure” or a “booster” to help me heal?
If you are struggling with a slow-healing jaw, research from 2024–2026 offers significant hope. We have moved toward actively restarting the healing process.
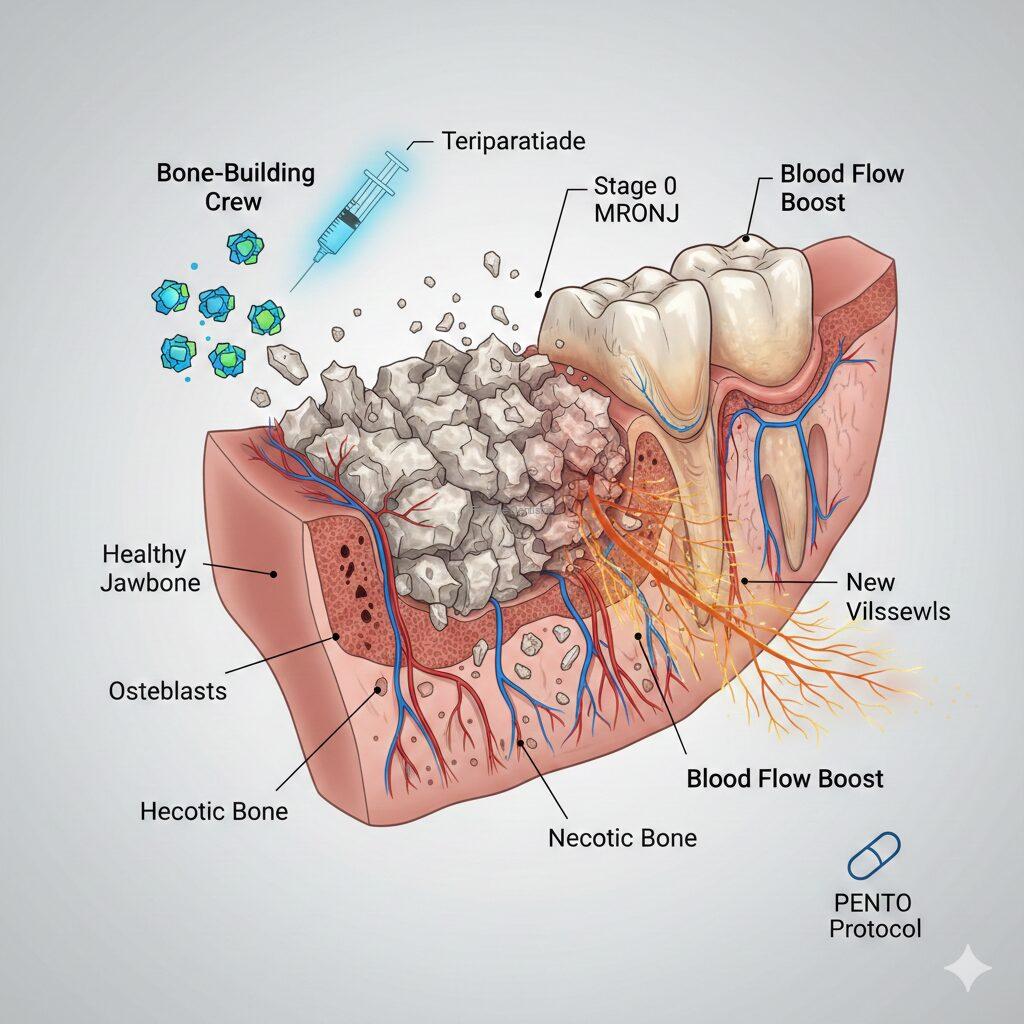
- The “Bone Builder” (Teriparatide/Forteo): The 2025 Korean Consensus confirms this is a game-changer for osteoporosis patients. It acts like a “new crew of workers” (osteoblasts) that build fresh bone. This “Self-Healing Effect” can sometimes push out dead bone on its own, helping you avoid major surgery.
- For Cancer Patients (PENTO Protocol): Since Forteo isn’t usually recommended for cancer patients, doctors use the PENTO Protocol (Pentoxifylline and Vitamin E). This “softens” scarred tissue and brings fresh blood supply back to the jawbone.
- The Future (Evenity/Romosozumab): The newest “kid on the block” in 2026 research. It is the most powerful bone-builder available and is being studied to provide an even faster “jumpstart” than Teriparatide.
6. If I get MRONJ, do I need surgery?
Yes, more than likely. In the past, the advice was “wait and see.” However, the 2022 AAOMS and 2025 international updates have shifted toward early active surgery. Removing the dead bone early often stops the condition from spreading and allows the healthy bone underneath to finally heal.
7. Can I still get Dental Implants?
- Osteoporosis Patients: Generally considered safe, but the 2024 Japanese update suggests extra caution if you have been on meds for over 3 years.
- Cancer Patients: High-dose IV medications usually make implants a high-risk choice that most international guidelines discourage.
8. What is the #1 thing I can do to prevent it?
Oral Hygiene. MRONJ is almost always triggered by infection. Both the Italian and Japanese papers highlight that meticulous brushing, flossing, and professional cleanings are your best defense. If you are about to start these medications, see your dentist first to get all “problem teeth” fixed.
References
- AAOMS (2022): Ruggiero SL, et al. American Association of Oral and Maxillofacial Surgeons Position Paper on MRONJ—2022 Update. J Oral Maxillofac Surg. 2022;80(5):920-943.
- Italian Consensus (2024): Campisi G, et al. SIPMO-SICMF Joint National Consensus on MRONJ: 2024 Update. Ital J Oral Med Pathol. 2024;15(1):12-34.
- Japanese Revised Paper (2024): Yoneda T, et al. Next-generation Japanese Position Paper on MRONJ: Revised July 2024. J Bone Miner Metab. 2024;42(4):401-425.
- Korean Consensus (2025): Kim JW, et al. 2025 Korean Multidisciplinary Position Statement on MRONJ. J Bone Metab. 2025;32(1):1-18.
- Sim et al. (2024): Teriparatide for MRONJ: A Randomized Controlled Trial. J Bone Miner Res. 2024;39(2):155-164.
- Owosho et al. (2024): PENTO Protocol in the Management of MRONJ: Updated 2024 Systematic Review. Head Neck. 2024;46(3):580-592.
Finesse Dental & Implant Center of Boston
617-286-6515 (Call/Text)
support@FinesseBoston.com
183 Essex St, Boston, MA
